
MCL Knee Ligament Injury
Medial Collateral Ligament — Inner Knee Stability
MCL injuries are among the most common knee injuries in sport and everyday life. Most recover well with the right physiotherapy — but recovery depends on an accurate diagnosis and a plan matched to your grade of injury.
Sports physiotherapy is one of the key strengths at Alleviate Physiotherapy. Whether your MCL injury happened on the soccer field, the ski hill, or from a misstep in daily life, our physiotherapists and chiropractors assess the full picture — the ligament, the surrounding structures, and your goals — before building a recovery plan tailored to you. We treat patients across Etobicoke, Mississauga, Clarkson/Oakville.
What is the MCL?
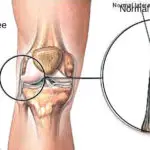
The medial collateral ligament (MCL) is a strong band of collagen tissue on the inner side of your knee. It connects the femur (thigh bone) to the tibia (shin bone) and acts as a guardrail — preventing the knee from bending excessively inward and resisting sideways forces during movement.
Ligaments do not stretch or contract like muscles. They act as sturdy structural straps that keep bones properly aligned across a joint. When the MCL sustains more force than it can handle, it stretches, partially tears, or tears completely — producing the pain, swelling, and instability that characterise an MCL injury.
The MCL vs. the Other Knee Ligaments
The knee has four primary ligaments. The MCL and LCL (lateral collateral ligament) sit on the sides of the knee, controlling sideways stability. The ACL and PCL (cruciate ligaments) cross deep inside the joint, controlling front-to-back movement and rotation. Each ligament protects a different plane of knee movement — and each requires a different assessment and treatment approach when injured.
Understanding All Four Knee Ligaments
Knowing where each ligament sits — and what it does — helps make sense of why different injuries present so differently and heal at different rates.
| Ligament | Location | Function | Healing Potential |
|---|---|---|---|
| MCL — Medial Collateral | Inner side of knee — outside the joint capsule | Prevents the knee from buckling inward | Good — often heals conservatively |
| LCL — Lateral Collateral | Outer side of knee — outside the joint capsule | Prevents the knee from buckling outward | Good — often heals conservatively |
| ACL — Anterior Cruciate | Centre of knee — inside the joint capsule | Controls forward shin movement and rotation | Poor — often requires surgical consideration |
| PCL — Posterior Cruciate | Centre of knee — inside the joint capsule | Controls backward shin movement | Poor — often requires surgical consideration |
Why the MCL and LCL Heal Better Than the ACL and PCL
The MCL and LCL sit outside the knee's joint capsule. This gives them a good blood supply and keeps them away from the synovial fluid inside the joint — fluid that contains enzymes that actively inhibit ligament healing. The ACL and PCL sit inside the joint, bathed in synovial fluid and with limited direct blood supply. Torn ACL and PCL fibres cannot receive the nutrients they need to knit back together — which is why these injuries often require surgical reconstruction rather than conservative rehabilitation alone.
What Causes an MCL Injury?
MCL injuries occur when the inner knee faces a force it cannot absorb. The most common cause is a direct blow to the outer side of the knee — pushing the joint inward and overstretching or tearing the MCL. They are most frequent in contact sports, but they can happen to anyone.
Common causes and risk factors include:
- Direct impact: A tackle, collision, or blow to the outer knee in contact sports such as football, soccer, basketball, or hockey.
- Cutting and pivoting: Forceful twisting of the knee during rapid direction changes — common in lacrosse, skiing, and basketball.
- Sudden stops: Decelerating quickly while running places large rotational and valgus forces through the knee.
- Awkward landings: Landing from a jump with the knee in a valgus (knocked inward) position.
- Hyperextension: Forcing the knee beyond its normal range of extension.
- Repeated stress: Overuse, previous knee injuries, or age-related wear and tear raise the risk of MCL strain under lower-force loads.
⚠ The "Unhappy Triad" — When Multiple Structures Are Injured Together
MCL injuries sometimes occur alongside other knee injuries — particularly ACL tears and meniscal damage. This combination, known as the "unhappy triad," produces considerably greater instability and requires a more intensive recovery plan. If your knee sustained a high-energy injury, your physiotherapist will assess all structures — not just the MCL — before confirming a diagnosis.
Recognising a Knee Ligament Injury — Symptoms by Ligament
Each of the four knee ligaments produces a slightly different symptom pattern when injured. This is not a substitute for professional assessment — but understanding the patterns helps you describe your symptoms clearly when you see your therapist.
MCL — Inner Knee Pain
Pain and tenderness along the inner side of the knee. Stiffness and swelling develop within hours. The knee may feel wobbly or unstable when changing direction. Occasional catching or locking during movement. Symptoms worsen with sideways stress on the joint.
ACL — Central Instability
A distinct "pop" at the moment of injury is common. Rapid, significant swelling — often within two to four hours. Difficulty bearing weight. A strong sense that the knee may buckle or give way. Reduced range of motion immediately after injury.
LCL — Outer Knee Pain
Pain, tenderness, swelling, or bruising along the outer edge of the knee. Discomfort when moving the leg sideways. The knee may feel unstable or as if it could give way during activity. LCL injuries are less common but often occur alongside other lateral knee injuries.
PCL — Posterior Knee Pain
Pain behind the knee — particularly noticeable when squatting, kneeling, or going downstairs. Swelling develops gradually and is typically milder than an ACL injury. A sense of looseness or instability, though often less dramatic than ACL symptoms.
Symptoms Alone Cannot Confirm a Diagnosis
Symptom patterns overlap significantly between ligament injuries and with other knee conditions — including meniscal tears, patellofemoral syndrome, and bursitis. A physiotherapist uses hands-on clinical tests to assess joint stability, ligament integrity, and movement quality. Imaging (MRI or X-ray) is recommended where the diagnosis is unclear or where combined injuries need ruling out. Do not attempt to diagnose based on symptoms alone.
Grades of MCL Injury — How Severe Is It?
MCL injuries classify into three grades based on the extent of ligament damage. Your grade determines the appropriate management approach and gives a realistic guide to your recovery timeline.
Grade 1 — Mild
A minor stretch or small tear of the ligament fibres. Some localised pain and tenderness, but the knee remains structurally stable. No significant loss of joint integrity. Recovery: typically 2–4 weeks with appropriate management.
Grade 2 — Moderate
A partial tear of the MCL. Moderate pain, swelling, and some joint instability — particularly on sideways stress. Walking is possible but uncomfortable. Recovery: typically 4–8 weeks, depending on associated injuries.
Grade 3 — Severe
A complete tear of the MCL. Significant pain, swelling, and clear knee instability. Other structures (ACL, meniscus) are often also involved. Recovery: typically 8–16 weeks; surgical consultation required in some cases.
How Can Physiotherapy Help with an MCL Injury?
The MCL has a good capacity to heal — but that healing needs the right environment and the right stimulus at each stage. Doing too much too soon re-stresses healing fibres. Doing too little slows remodelling and risks incomplete recovery. The right balance — and the right sequence of interventions — is what physiotherapy provides.
Both physiotherapy and chiropractic care play a vital role in MCL rehabilitation. Their techniques differ, but both aim to promote healing, reduce pain, restore function, and improve overall musculoskeletal health. At Alleviate Physiotherapy, your care team brings both disciplines together under one roof.
We follow our signature three-step approach:
Assess
A thorough hands-on evaluation of the knee — ligament integrity, joint stability, range of motion, strength, and movement quality — to confirm the diagnosis and grade before treatment begins.
Alleviate
The type of diastasis, the degree of functional impairment, pelvic floor involvement, and the specific activities driving strain.
Achieve
Progressive strengthening, proprioception training, and sport-specific rehabilitation to return you to full activity — stronger and more resilient than before.
Physiotherapy Treatment — Phase by Phase
Treatment adapts as your knee heals. What your therapist prescribes in week one looks very different from week six. The following phases outline the typical progression — your therapist adjusts timing and content based on your grade of injury and your response to treatment.
Phase 1: Acute Management (Days 1–14)
Assessment and Diagnosis
Your physiotherapist assesses the extent and severity of the MCL injury, tests for associated damage to the ACL, meniscus, and other structures, and determines the appropriate management pathway. MRI or X-ray referral is arranged where needed to confirm the diagnosis or rule out combined injuries.
Pain and Swelling Management
Ice, compression, elevation, and offloading reduce acute swelling and pain. Your therapist may use therapeutic ultrasound, electrical stimulation (TENS or NMES), or manual lymphatic techniques to accelerate this process. Appropriate bracing or support is fitted where instability warrants it.
Protected Mobility
Early, gentle range-of-motion exercises prevent stiffness and promote circulation to the healing ligament — without stressing the repair. Your therapist determines the appropriate degree of motion and weight-bearing for your grade of injury. Immobilisation beyond the minimum necessary slows recovery.
Phase 2: Restoration of Movement and Strength (Weeks 2–6)
Range of Motion and Flexibility Work
Targeted exercises restore full knee flexion and extension. Manual therapy — including joint mobilisation (Maitland technique), soft tissue release, and Mobilization with Movement (MWM) — addresses residual stiffness and improves joint mechanics as the ligament heals.
Progressive Strengthening
Graded exercises rebuild the quadriceps, hamstrings, glutes, and calf muscles that support and protect the healing MCL. The progression follows your pain levels, swelling response, and movement quality — not a fixed calendar. Advancing too quickly under load risks re-injury to the healing ligament.
Manual Therapy and Soft Tissue Work
Hands-on techniques reduce scar tissue formation around the MCL, improve joint mobility, and address associated muscle imbalances that may alter knee mechanics. Chiropractors at Alleviate may use active release therapy, myofascial release, or IASTM (instrument-assisted soft tissue mobilisation) as part of this phase.
Phase 3: Proprioception, Balance, and Functional Return (Weeks 4–12)
Balance and Proprioception Training
MCL injuries disrupt the proprioceptive nerve endings within the ligament — the sensors that tell the brain where the knee is in space. Specific balance and neuromuscular exercises retrain these pathways. This step directly reduces the risk of re-injury, as many knee re-injuries occur not from inadequate strength but from impaired joint position sense.
Sport-Specific and Functional Rehabilitation
Running mechanics, cutting, pivoting, jumping, and landing are progressively reintroduced under therapist supervision. Exercises mimic the specific demands of your sport or activity. Criteria-based return to sport — not time alone — determines when it is safe to resume full participation.
Prevention Education and Movement Retraining
Your physiotherapist identifies the movement patterns, biomechanical risk factors, and training habits that contributed to your injury. Corrective strategies, postural advice, and a structured prevention programme reduce your risk of re-injury when you return to sport or full activity.
When Is Surgery Considered?
Most MCL injuries — including complete Grade 3 tears — respond well to conservative management with physiotherapy and bracing. Surgery for an isolated MCL tear is relatively uncommon.
Surgical consultation becomes relevant in these situations:
- The MCL tear accompanies a significant ACL, PCL, or meniscal injury requiring surgical repair.
- Conservative treatment over an appropriate period fails to restore knee stability.
- Chronic instability continues to affect daily activities, work, or sport.
- The patient has a high activity level with significant demands on knee stability — such as competitive athletes in pivoting sports.
ACL and PCL Injuries Often Require a Different Conversation
Unlike the MCL, a torn ACL or PCL rarely heals on its own. Their location inside the knee joint — surrounded by synovial fluid with limited blood supply — means the torn ends cannot receive the nutrients needed to repair. If imaging or clinical testing suggests ACL or PCL involvement alongside your MCL injury, your physiotherapist will discuss the full picture with you and refer appropriately. Many people function well after ACL injury without surgery — but that decision requires a full assessment of your activity demands and functional goals.
What to Expect When You Come to See Us
If you think you have injured a knee ligament, the first step is a professional assessment. Do not try to determine which ligament based on symptoms alone — the patterns overlap, and missing a combined injury can significantly affect your recovery.
Here is what your experience at Alleviate Physiotherapy looks like from first contact to full recovery:
Initial Assessment
A detailed clinical examination covering your symptom history, hands-on ligament stability tests, movement assessment, and strength testing. Imaging referral is arranged where clinical findings indicate it. You leave your first appointment with a clear diagnosis, a grade, and an outline of your treatment plan.
Personalised Rehabilitation Plan
Your plan reflects your grade of injury, your activity goals, and your lifestyle. It progresses through clear phases — from pain management to full functional return. You know what you are working toward at each stage and why.
Transparent, Ongoing Communication
Your therapist explains what is safe to do at each stage, what to avoid, and what progress markers indicate it is time to advance. Your plan adapts as your knee responds — not on a fixed calendar.
Referral When Needed
If your injury requires orthopaedic surgical input, advanced imaging, or specialist review, our team connects you to the right person. Your physiotherapy care continues alongside any specialist pathway — not instead of it.
Your Questions Answered
Symptom patterns give useful clues — but a proper clinical assessment is the only reliable way to confirm which ligament is involved. Each ligament tends to produce pain in a different location: the MCL on the inner knee, the LCL on the outer knee, the ACL centrally with a "pop" and rapid swelling, and the PCL behind the knee with pain on squatting or kneeling.
The problem is that these patterns overlap — and combined injuries (such as ACL plus MCL) are common. A physiotherapist uses specific stability tests for each ligament to confirm the diagnosis. MRI is recommended where clinical findings are inconclusive or where multiple structures may be affected. Book an assessment before drawing any conclusions.
Yes — the majority of MCL injuries at all three grades recover well without surgery. The MCL's location outside the joint capsule gives it a reliable blood supply and keeps it away from the healing-inhibiting enzymes found in synovial fluid. With appropriate bracing, physiotherapy, and time, even complete Grade 3 tears often heal to full functional stability.
Surgery for an isolated MCL tear is uncommon. Where surgery does become relevant is when the MCL injury accompanies damage to the ACL, PCL, or meniscus — or when conservative management over an appropriate period fails to restore adequate stability. Your physiotherapist will assess whether your injury is isolated or combined and advise accordingly.
Recovery time depends primarily on your grade of injury and whether other structures are involved. As a general guide: Grade 1 injuries typically resolve in 2–4 weeks. Grade 2 injuries take 4–8 weeks. Grade 3 injuries require 8–16 weeks or longer, particularly where combined injuries need management.
These are guidelines — not guarantees. How quickly you advance through rehabilitation phases depends on how your tissue responds to treatment, how consistently you complete prescribed exercises between sessions, and whether you remain within safe loading limits during recovery. Your therapist sets criteria-based milestones rather than calendar-based targets.
Yes — and it is more common than many people expect. The "unhappy triad" — simultaneous damage to the ACL, MCL, and medial meniscus — is a well-recognised injury pattern in contact sports involving twisting impacts. High-energy injuries to the knee should always be assessed for combined ligament damage.
Combined injuries are more complex to manage and typically require longer recovery timelines. In some cases, the presence of an ACL or PCL injury alongside an MCL tear changes the surgical decision significantly. A thorough clinical assessment — and often an MRI — is essential to identify all structures affected before deciding on a management pathway.
The ACL sits inside the knee joint, surrounded by synovial fluid. This fluid contains enzymes that actively interfere with the ligament healing process. The ACL also has a limited direct blood supply compared to the MCL. When torn, the ACL ends cannot receive the nutrients and cellular building blocks needed to knit back together.
The MCL, by contrast, sits outside the joint capsule with a good blood supply and no exposure to synovial fluid. This is why the MCL typically heals well conservatively while a torn ACL generally does not — and why the two injuries, though they can occur together, follow such different treatment and recovery pathways.
As soon as possible. Early assessment and appropriate management consistently produce faster and more complete recovery than delayed treatment. In the first 24–72 hours, your physiotherapist can confirm the diagnosis, rule out fractures or combined injuries, begin protecting the healing tissue, and start the rehabilitation process — preventing unnecessary stiffness and deconditioning from developing while you wait.
Do not wait until the swelling has fully resolved or until pain makes daily activities impossible before seeking assessment. Earlier assessment means earlier clarity on what you are dealing with — and earlier clarity means a better recovery.
Signs You Should Book an Assessment Now
Do not delay seeking care after a knee injury. The earlier a physiotherapist assesses the damage, the better the recovery trajectory. Book an assessment promptly if any of the following apply:
- Inner, outer, or posterior knee pain that followed a direct impact, twist, or awkward landing.
- Rapid swelling within the first few hours of injury — a sign of significant tissue damage requiring early assessment.
- A "pop" at the moment of injury — associated with ACL injury until proven otherwise.
- Difficulty bearing weight or a strong sense that the knee may give way.
- Pain or instability that persists more than 48–72 hours after injury despite rest and ice.
- A previous knee ligament injury — prior damage significantly increases re-injury risk and warrants proper assessment rather than self-management.
Get Clarity on Your Knee — Then Get Better
A knee ligament injury needs an accurate diagnosis before it needs treatment. Our physiotherapists will assess every relevant structure, determine exactly what you are dealing with, and build a recovery plan that gets you back to the activities you love — stronger and more resilient than before.
Conveniently located across four GTA locations — Etobicoke, Mississauga, Clarkson/Oakville.
Reference: Brotzman, S.B. & Wilk, K.E. (2003). Clinical Orthopaedic Rehabilitation, 2nd ed. Mosby Publication. | Copyright © 2025 Alleviate Physiotherapy.
-
 ACL Injury – Physiotherapy and Chiropractic Care
ACL Injury – Physiotherapy and Chiropractic CareACL Injury – Physiotherapy and Chiropractic Care What is ACL Injury? ACL stands for Anterior Cruciate Ligament. Wear and tear...
-
 Baker’s Cyst
Baker’s CystKnee Conditions Baker’s Cyst That Mystery Lump Behind Your Knee A Baker’s cyst is rarely the real problem — it...
-
 Iliotibial Band Syndrome
Iliotibial Band SyndromeIliotibial Band Syndrome Pain in the outer thigh that affects your knee? Come visit one of our centers at Clarkson...
-
 Knee Osteoarthritis
Knee OsteoarthritisKnee Osteoarthritis Knee Osteoarthritis Suffering from Knee Osteoarthritis? Come see a Physiotherapist Near You!! Alleviate Physiotherapy isnow located in Oakville...
-
Knee Pain
Knee Pain Knee Pain? Suffering from a painful knee? Sprain/Strain? Osteoarthritis? What is Knee Pain? Any swelling, locking, popping, instability...
-
 LCL Injury
LCL InjuryLCL Injury Having a bad knee? It could be one of your ligaments. Come visit Alleviate Physiotherapy at Clarkson (...
-
 MCL Knee Ligament Injury
MCL Knee Ligament InjuryKnee Conditions MCL Knee Ligament Injury Medial Collateral Ligament — Inner Knee Stability MCL injuries are among the most common...
-
 Patellar Tendonitis
Patellar TendonitisPatellar Tendonitis Physiotherapy for Patellar Tendonitis aka Jumper’s Knee Are knee extensions painful? Can’t pin-point your knee pain to a...
-
PCL Injury
PCL Injury Have a PCL Tear? Here’s how top-rated physiotherapy can help Suffering from a painful knee? Sprain/Strain? Osteoarthritis? What...
-
 Runner’s Knee
Runner’s KneeKnee Conditions Runner’s Knee Patellofemoral Pain Syndrome (PFPS) — Expert Treatment at Alleviate Physiotherapy Is a sharp ache behind your...











